

International Hyperbaric Medical Association Witness
Paul G Harch MD, IHMA President
Mr. REGULA: Okay, we’ll get started, because we have a long list today, and we’ll probably get some interruptions for votes.
We’re happy to welcome all of you. These are important issues. I just came from my office full of people with diabetes. And they’re convinced that, maybe so, another couple of dollars and there will be a cure. I’m sure you feel the same way about whatever you’re dealing with.
The United States has done a remarkable job in research. I was impressed the other day; the NIH people testified that every five years, life expectancy goes up a year. So in 50 years, that’s 10 years. And that’s thanks to the research that’s done and a lot of what’s happening, good diet and a lot of things that are pluses.
Well, we want to get started, because we want to give everybody an opportunity. Our first witness will be introduced by David Vitter, from the great State of Louisiana.
Mr. VITTER: Thank you very much, Mr. Chairman. I’m pinch hitting today for Ernest Istook, but I’m very, very happy and honored to introduce Dr. Paul Harch from Louisiana. He’s an emergency and hyperbaric medicine physician who graduated magna cum laude and phi beta kappa from the University of California Irvine in 1976 with a bachelor’s degree in biology and subsequently from Johns Hopkins Medical School in 1980. He completed two years of general surgery training at the University of Colorado, one year of radiology at LSU School of Medicine, has worked 17 years in hospital based emergency medicine and 15 years in hyperbaric and diving medicine.
His primary interests have been brain decompression sickness and hyperbaric oxygen therapy, base-spec brain imaging index neuro-rehabilitation. He is going to obviously talk more about his work. It has been very, very promising, having treated over 180 children and 320 adults. And he’s now recognized as one of the foremost authorities in the U.S. on hyperbaric oxygen therapy.
In that capacity, he’s been elected as the first president of the newly formed International Hyperbaric Medical Association. And with that, I’m very pleased to present Dr. Harch.
Mr. REGULA: Dr. Harch, thank you for coming. Let me say to all of you, because we have 25 witnesses today, we have to limit you to five minutes. I’m sorry, but there just isn’t any choice. And there’s a little box on the desk that gives you a warning when the time is about to expire. If I ask questions, that’s on my time.
Dr. HARCH: Thank you Chairman Regula and members of the Committee, I first want to thank you for the opportunity to testify today. My name is Paul Harch, and as Mr. Vitter said, I am an emergency and hyperbaric medicine physician who is here representing the International Hyperbaric Medical Association and brain injured Americans. I’m not here to ask for money. I’m here to show you how we can save money and improve the health, welfare and outcomes of brain injured Americans.
What I’d like to say is that simply, we have a treatment for brain injury that is–
Mr. REGULA: All types of brain injury?
Dr. HARCH: Almost all types. We have looked at this now in over 500 patients over the last 12 years and 50 different brain based neurological conditions. This is a generic treatment for brain injury with, I believe, the capacity to revolutionize the treatment of brain injury in the world.
Amongst these 500 patients have been 180 children. The first five brain-injured children in the United States treated with hyperbaric oxygen therapy were treated by me in New Orleans. Many of these children have cerebral palsy, autism, near-drowning, a variety of neurological disorders. And many of them include IDEA children, who as you know, the Federal and State Government is now spending $55 billion a year to attempt to educate, when they don’t have the capacity to learn, often from organic brain injury.
This treatment, as we have shown in a number of these children, can give them the capacity to learn. And the cost is roughly about a year to a year and a half of the education support money.
What I wanted to show you today was that this can be applied in a variety of conditions. After presenting this in 1992 through 1995 to scientific meetings and experiencing a fair amount of criticism, I went to an animal model. We have now done this and replicated this in animals and have the first-ever demonstration of improvement of chronic brain injury in animals.
What I wanted to show you today and just mention quickly about diabetes, this is actually the only modality that can prevent major amputations in diabetics with foot wounds, which as you know is a major failed target of the Healthy People 2000 initiative. What I’m going to show you here today is, there are a few examples of what can be done.
And the patient here, whose brain scans are on the poster, is one of Mr. Istook’s constituents. This is the first Alzheimer’s patient in the United States and possibly the world treated with hyperbaric oxygen therapy for his Alzheimer’s. He was a 58 year old architect who of course had lost his job and now needs 24 hour supervision
and accompaniment by his wife.
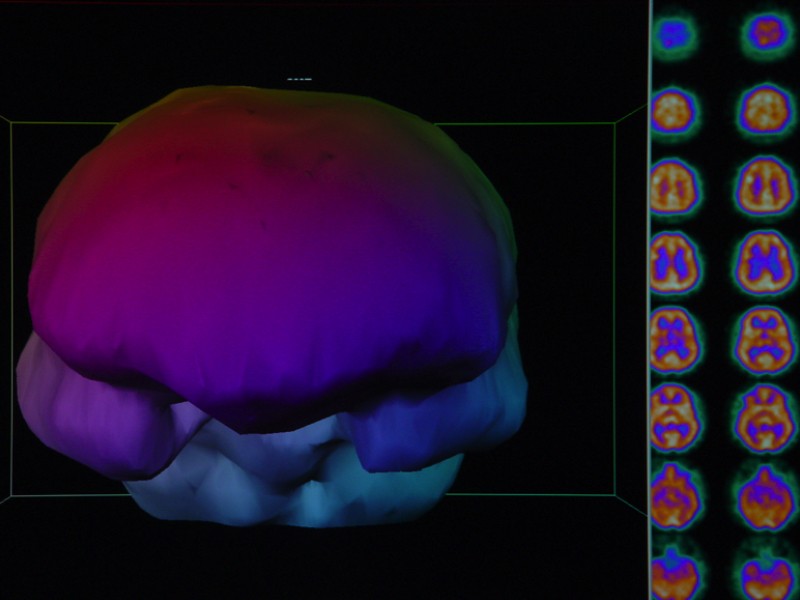
After a lecture I gave at the University of Oklahoma Health Science Center, the neurology group referred him as a test case. What you’re looking at here are brain blood flow scans. The way brain blood flow in the brain works is similar to a gasoline engine. More gasoline, more blood flow, more RPMs to the engine, better metabolism to the brain.
If you look at these pictures, these are three dimensional reconstructions of the human brain blood flow. On top here is the brain scan before treatment and this is the face view. We’re looking right at the patient. The eyes would sit here, and wherever there are holes in the brain are significant reductions in blood flow. This is the right side view and this is the left side view, and here is the top view. Where the three major arteries in the brain on each side come together is right here, on each side. That’s the most vulnerable area for brain injury. It’s the area primarily injured in Alzheimer’s.
After three and a half months of treatment, 89 hyperbaric treatments, you see how all of these damaged areas of the brain have begun to fill in. Simultaneously, he was tested by the neuropsychologist at University of Oklahoma–
Mr. REGULA: We’ve got about a minute left. Tell me what the process is.
Dr. HARCH: It is putting a patient in an enclosed chamber, increasing the pressure and giving them pure oxygen. It dissolves in the blood and you’re able to put the oxygen in the liquid portion of the blood, above and beyond what is bound to hemoglobin in our red blood cells, which as you and I now have, 100 percent saturation. It’s then delivered to injured areas in the body, and by repetitive exposure, you grow new blood vessels, you stimulate damaged cells to begin repair.
Mr. REGULA: Because there’s a more intense flow of oxygen to the injured, in this case the brain area.
Dr. HARCH: Exactly. And it’s an ability to restore, not dead, but damaged tissue that is not functioning.
Mr. REGULA: Okay. You developed the process. It is being used or is it still in an experimental stage?
Dr. HARCH: It is being used for a variety of other indications. And increasingly so for this, at a number of centers in the United States.
Mr. REGULA: Has NIH done any experimentation with this?
Dr. HARCH: No. Well, there has been some in the past, on senility and some other neurological disorders.
[The prepared statement of Paul G Harch MD follows:]
Testimony
“The Impact of Hyperbaric Medicine on Government Health Care, Disability and Education Expenditures”
The International Hyperbaric Medical Association
Paul Harch, M.D.
President
Before the
Labor, Health and Human Services and Education Subcommittee
Of the Committee on Appropriations
United States House of Representatives
May 2,2002
Chairman Regula, Mr. Obey, and distinguished members of this committee, lam Dr. Paul Harch, President of the International Hyperbaric Medical Association, and a resident of Louisiana. Bob Livingston was my Congressman. Two years ago, Mr. Istook of Oklahoma started the Hyperbaric Oxygen Initiative at the National Institutes of Health. Many of his constituents have become my patients, one of whom I will present today for the first time in a public setting.
We were all taught that brain cells don’t regenerate. Four years ago, NIH announced to this panel that medicine had been in error all of these years and challenged the medical community to begin searching for a way to do so. Hyperbaric Medicine has been repairing brain injuries right here in America for 30 years, but no one would look at it because everyone “knew” that it was not possible.
Hyperbaric oxygen therapy (HBOT) involves the delivery of $7 worth of oxygen in a pressurized environment created by a chamber. Some of these chambers are the size of this table, and others are the size of a small room. The pressure serves to saturate the tissues of the body, not only the hemoglobin in the blood, but the plasma, lymph and cerebral spinal fluid, all of which go many places that hemoglobin cannot reach, especially in cases of traumatic injury. The average treatment takes I to I Y, hours and Medicare reimburses at $75 per Y. hour of treatment, plus a $35 physician attendance fee.
Bob Moffitt, Director of Domestic Policy at the Heritage Foundation said, “Congress should authorize an intensive evaluation of Hyperbaric Oxygen Therapy with a view in order to determine its cost effectiveness and its contributions to high quality care.” It is in the federal government’s financial interest to do so.
I know you have many conflicting priorities Mr. Chairman, and Ms. Pelosi has often said this committee’s decisions often involve “the lambs eating the lambs.” Unlike many who have testified before the committee, I am not here asking for more money, I’m here to save you money. In the words of one distinguished public health official, “zillions of dollars.” This money could be used to fund other pressing priorities and even return some to the taxpayers.
Let me give you a few examples.
Forty percent of my practice is neurologically injured children. You would consider them IDEA children, who cost on average, 2.1 times as much to educate as a non-injured child. There are 6.548 million IDEA children in the nation, and this year the President has asked for a budget of $8.5 billion to pay for 18 percent of the obligations of the federal government to the states. These children are costing the state’s educational system $47 billion, for a total of$55.7 billion. On average, nationally, they cost $8,510 more per year to educate than a “normal” child. Many cannot learn due to their injuries. The therapy I am here discussing would cost an average, one time expenditure of between $7,000 and $14,000 for most children treated long after the injury, the cost of educating them for a year or two. The effects would be permanent and last throughout their lifetime. For many of these children, if they had been treated immediately upon injury, the costs drop to often less than $1,000. [Pages 4, 5, 6, 8, 10, 15, 17]
Many of these children have neurological injuries that affect their motor skills, learning, speech, etc. They are children injured in birth trauma, accidents, child abuse, fetal alcohol syndrome, maternal drug use, or other such events. Current practice deals with the brain that is still there and tries to re-train it. The therapy we are discussing has effectively recovered and rebuilt brain tissue through reactivation of stunned tissue, revascularizeation and, possibly, stimulation of adult stems cells in the brain to repair existing neural pathways and grow new ones.
Follow many of these children into adulthood, and you discover that many wind up in prison, on welfare, Social Security Disability, in long-term care facilities at state or insurance company expense or become a drain on the system in some other fashion. Many of these children suffering from Mental Retardation or Developmental Disabilities, when they grow to adulthood, cost, on average, $43,000 per year in group home or institutional settings. (3.8 million, 59% under 17, 38% between 17 & 64) My hyperbaric medical practice has demonstrated that nearly all of these children can be helped, including many with genetic disorders, and many, many, can lead full, normal and productive lives. This is something current medical practices cannot provide for most of them. [Page 9]
I also serve as a prison physician, and can tell you that many prisoners suffer from a neurological injury incurred prior to incarceration and seizure disorders secondary to those injuries. The injury often drives their violent and irrational behavior. The Department of Justice has reported that up to 20% of the inmates report some type of mental impairment. In New Orleans, Louisiana we have a substantial number of our 7,500 inmates in our prison population with seizure disorders. Many ore have experienced head trauma. [Page 13]
Hyperbaric medicine significantly affects other areas of your committee. For example, in patients with diabetic foot wounds, hyperbaric oxygen has been shown to decrease major amputations by over 75%. There are currently 54,000 amputees on the Social Security Disability Income or SSI roles, at an average cost of$8,467 per year. Many of these amputations could have been prevented through acute and chronic treatment of their medical condition with Hyperbaric Oxygen prior to amputation. Congressman Istook’s Deaconess Wound Care Center has less than a 1% amputation rate for those who receive Hyperbaric Treatment. CMS is deciding in 90 days whether amputations or treatment with Hyperbaric Oxygen is more cost effective. All of the other major insurance companies, including Blue Cross/Blue Shield already pay for diabetic wound treatment.
In addition, the latest JAMA article on heart by-pass surgery showed that 30% of those undergoing this procedure have residual brain damage, which could be largely solved by a single $225 Hyperbaric treatment. Further treatments applied under a surgical protocol could possibly heal patients between 25% and 50% faster, concurrently reducing costs to the insurance company, the government, malpractice insurance and physicians time and fees. The Navy has applied HBOT to fractures and returned many soldiers to duty who would have otherwise been discharged from service, saving the VA hundreds of thousands over the life of a veteran.
In the year 2000, the government spent 5.5 billion Medicare dollars on strokes, or $3,169 per patient, with little hope of full recovery. Hyperbaric medicine, especially acute treatment, cost effectively offers many such hope. Even chronic stroke patients can experience significant improvement in function and quality of life. [Pages II, 12]
Social Security disability currently has 61,500 brain injured people on the Disability or SSA roles at a cost of$8,459 per person per year. Many of these people could be returned to full and productive lives.
One of Mr. Istook’s constituents is the first person to start the true return from early onset Alzheimer’s disease. I know the Committee has great interest in this dread disease. (Page 7)
Let me illustrate what I’m talking about with real, live patients. I believe it will demonstrate what I am discussing today.
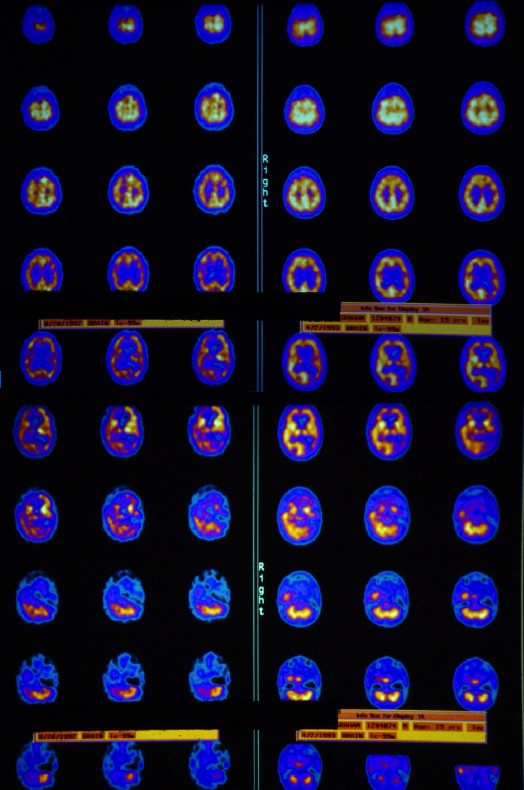
[Discussion of Slide Presentation Handout with SPECT Scans. Download the PDF Here]
Page 4: Acute & Chronic Treatment of Traumatic Brain Injury & Coma – 19-year-old male
Page 5: Traumatic Brain Injury and Substance Abuse – 23 year old male
Page 6: Traumatic Brain Injury – 23 year old female
Page 7: Alzheimer’s Disease – 58 year old male
Page 8: Physical Abuse & Rape – 21 year old female
Page 9: Mental Retardation – 44 year old male
Page 1 0: Cerebral Palsy – 8 year old male
Page 11: Stroke – 60 year old male
Page 12: Alcoholism and Stroke – 68 year old male
Page 13: Substance Abuse – 19 year old male
Page 14: Carbon Monoxide Poisoning- 51 year old female
Page 15: Shaken Baby- 6 month old female
Page 16: Gun Shot Wound to the Brain – 29 year old female
Page 17: Autism- 3 year old female
Page 18: Traumatic Brain Injury from Child Abuse – 48 year old male
I would encourage you to fully support Mr. Istook’s Hyperbaric Oxygen Initiative language (attached), and encourage the National Institutes of Health, the Centers for Disease Control, the Agency for Healthcare Research and Quality, the Centers for Medicare and Medicaid Services, the Health Resources Services Administration, the Substance Abuse and Mental Health Services Administration, the Social Security Administration and others to get the word out that $7 worth of oxygen, delivered at pressure, will save money, save lives, and improve the quality of life for millions of Americans, and provide hope to many who live lives of quiet desperation.
I welcome the opportunity to answer any questions the committee has.
Representative Ernest Istook, Report Language for National Institutes of Health, FY 2003, Hyperbaric Oxygen Initiative
In accordance with report language from the Committee in previous years, the Office of the Director is encouraged to coordinate a hyperbaric Oxygen research initiative in coordination with the International Hyperbaric Medical Association, the American College of Hyperbaric Medicine, and the Undersea and Hyperbaric Medical Society. The NIH is encouraged to work with these three groups to examine widespread use of hyperbaric oxygen therapy for various manifestations of reperfusion injury, such as in organ transplantation, limb reattachment, and before and after surgical procedures involving tourniqueting of extremities: peripheral arterial bypass procedures, amputations, orthopedic procedures, plastic surgery procedures, flap and graft procedures, etc. Investigation of this treatment for hemorrhagic shock, multiple trauma injury and multiple trauma crush injury is also indicated based upon animal and clinical research already conducted. Such an initiative should also include the examination of the results of a single before and after hyperbaric treatment for surgery patients. The treatment of surgery patients in this manner could result in significant cost reductions and both long-term and short-term results should be examined.
In addition, the International Hyperbaric Medical Association has extensive expertise in the use of hyperbaric oxygen treatment for acute, subacute, and chronic brain injuries, such as traumatic brain injury, stroke, toxic brain injury, brain injuries from substance abuse, air embolism, dementia (including Alzheimer’s disease), carbon monoxide poisoning, pediatric neurological injury (which would include autism, cerebral palsy, and multiple other childhood neurological disorders), and the broad spectrum of neurological disease. The office of the director is encouraged to work with researchers from this association to explore the short- and long-term cost reduction impact of low pressure hyperbaric oxygen therapy for these chronic disabling neurological conditions. In addition, the office of the director is requested to explore the cost-saving potential and improved efficiency of single hyperbaric oxygen therapy treatments before and after cardiac surgery which involves heart-lung bypass, and hyper acute hyperbaric oxygen therapy for the entire group of brain injuries that follow global ischemia and anoxia and which are characterized by reperfusion injury. This group of brain injuries includes near drowning, near-banging, cardiac arrest, electrocution, suffocation, anesthesia anoxia, perinatal brain injuries (resuscitation at birth, birth apnea, etc.), and other acute brain injuries resulting from cessation and subsequent resumption of cerebral blood flow. The initiative should examine both the clinical applications of these methods and the underlying mechanisms of action taking place as a result of this inexpensive treatment.
The NIH Director is encouraged to coordinate this initiative across all the appropriate institutes.